Sotos syndrome: symptoms, causes and treatment
Sotos syndrome is a genetic disease affecting skull development.
Children with a bone age 2, 3 or even 4 years older than their chronological age, large hands and feet, sucking problems and some problems in their cognitive, social and motor development.
These are the main characteristics of Sotos syndrome, a medical condition of genetic origin that is quite common in the population, although it is not very well known.
People who suffer from it end up developing more or less normally, although at the wrong time. In the following we will discover more about this strange but, at the same time, frequent syndrome.
What is Sotos syndrome?
Sotos syndrome is a medical condition of genetic origin that is characterized by excessive intrauterine or postnatal growth accompanied by delayed motor, cognitive and social development.. Children with this syndrome are significantly larger than expected for their age, although their weight is in accordance with their height. In addition, newborns show excessive growth in the bones, hands and feet and some characteristic facial features.
Unlike many genetic diseases, Sotos syndrome may not be evident at birth, requiring months or even years to be properly diagnosed. As they approach adolescence, sufferers approach a development closer to normal, and in adulthood may have intellectual, behavioral and motor skills appropriate for their social environment.
This syndrome is named after Dr. Juan Sotos in 1964, a specialist in pediatric endocrinology. who described 5 children with learning problems, overgrowth and characteristic appearance, calling it for the first time cerebral gigantism. However, not all the merit is attributable to Sotos, since Dr. Bernard Schelensinger described in 1931 a patient whose symptoms were consistent with this syndrome, being the first known description of the syndrome.
Apparently, is one of the most common overgrowth syndromes.. Although the true incidence has not been assessed, it is estimated that between 1 in 10,000 and 50,000 live births have this syndrome, although the safest estimate is 1 in 14,000 births. It is probably the second most frequent overgrowth syndrome, after Beckwith Wiedemann syndrome.
Causes
The exact causes of the syndrome are unknown, but it is clear that its origin is genetic. it is clear that its origin is genetic, being autosomal dominant inheritance..
In 2002 it was discovered that on chromosome 5, mutations and deletions in its NSD1 gene could be behind Sotos syndrome (5q35 deletion). This gene is a histone methyltransferase involved in transcriptional regulation. About at least 75% of Sotos cases present this gene alteration.
Characteristics of the syndrome
There are several defining features of this syndrome. The main symptom is the rather rapid growth during the first 5 years of life, in addition to having an advanced bone age.. The children present a size and weight according to children 2 or 3 years older than them. Once they reach 10 years of age, children with Sotos syndrome have a height of 14 or 15 years old adolescents, reaching the height of an adult much earlier than expected.
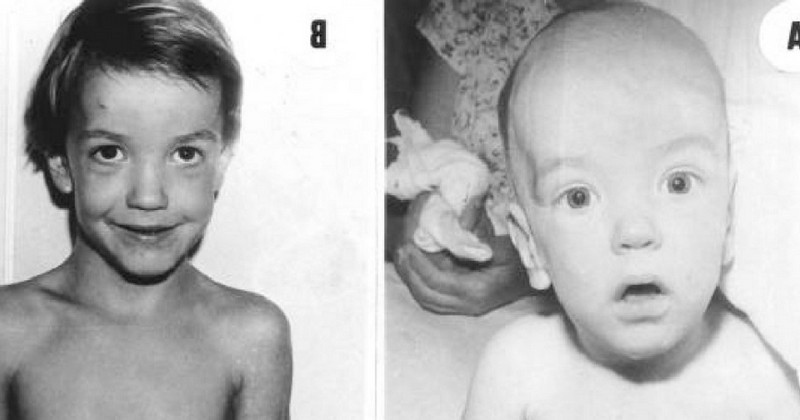
At birth, the following can be observed the presence of a highly arched palatewhich causes the baby to have difficulty sucking and this causes feeding problems, which can lead to jaundice. Their head is usually large, presenting macrocephaly, prominent forehead and chin. They may also present dolichocephaly, that is, an elongated skull. This is due to exaggerated enlargement of the brain tissue, which causes retention of cerebrospinal fluid in the ventricles.
The forehead is domed, and they may have ocular hypertelorism, i.e., the eyes are wide apart.. There are palpebral fissures, that is to say, folds are formed by the inclination of the eyelids downwards. The nasal bridge is flat, and the nose is anteverted. The cheeks and nose are flushed. The ears are protruding and large, and the hairline is receding. The teeth develop prematurely, in accordance with their overgrowth.
They have disproportionately large hands and feet compared to the rest of the body, as well as flat or collapsed feet. Their spine may tend to suffer deviations that, if chronic, will lead to scoliosis. All of this is accompanied by muscular hypotonia, giving rise to motor delays and motor retardation.resulting in motor delays and difficulty in movement. This also affects the face, since the tone of the facial muscles is low, producing prolonged drooling and having to breathe through the mouth.
People with Sotos syndrome often show signs of restlessness, hyperactivity and aggressiveness. In addition, there may be intellectual disability, although in a very variable way, aggravated by difficulties in language development. It should be said that the language problems are due to the arched roof of the palate. In any case, all these psychic characteristics hinder integration in different social environments.
Although the person may have problems during the first years of life, the differences with respect to people without the syndrome begin to reduce in pre-adolescence. Muscle tone improves, which facilitates swallowing and speech, and motor, cognitive and social delays are reduced to the point of disappearing in many cases. This is why Sotos syndrome is considered by many to be a simple alteration in developmental timing rather than a type of disability..
There are other traits that are also related to the syndrome, although they are less common. These include dysfunctional behavior patterns, phobias, obsessions, aggressiveness and adherence to routine. There are cases of children with high memory capacity and autistic behaviors, similar to Asperger's, as well as hyperactivity.
There appears to be increased susceptibility to ear infections, respiratory problems such as Asthma and allergy, as well as increased risk of tumors and seizures. There may be delayed sphincter control and cardiac abnormalities, directly related to muscular hypotonia.
Diagnosis
A fundamental aspect in the diagnosis of Sotos syndrome is to make sure to perform an adequate differential diagnosis, making sure that it does not involve others with similar characteristics. Among the diseases that can be confused with this syndrome are Fragile X syndrome, Weaver syndrome and Marfan syndrome, very similar to Sotos syndrome but with more severe long-term consequences.
There are no specific tests for its diagnosis, which is based mainly on the recognition of physical features.. However, different tests can be used to confirm the diagnosis. X-rays of the hand and wrist can be used to determine the maturity of the bones, detecting an advancement of 2 or 3 years. Computed tomography (CT) of the brain can be used to see if the ventricles are abnormally large.
Other tests, to rule out other possible causes of the clinical picture, are hormone measurements and karyotypingi.e. a study of the patient's chromosomes. If an alteration in the NSD1 gene is detected, it is possible to be sure that it is a case of Sotos syndrome. At present it is not possible to make a diagnosis before birth.
Treatment
The treatment of Sotos syndrome is aimed at making the social, cognitive and motor development of the child as close to normal as possible.. Thus, many techniques are applied to facilitate the child's relatively normal development, such as early stimulation, occupational therapy, physical therapy, speech therapy and physical education. In a structured environment, the child is able to practice necessary skills without too many distractions.
As mentioned above, these children may present behavioral problems, such as restlessness, aggressiveness and hyperactivity. This hinders their ability to concentrate and hinders learning. For this reason, and given that the origin of these symptoms is biological, pharmacological treatment is often used. Among the most commonly used drugs we have methylphenidate hydrochloride, which is also used in ADHD.
Bibliographic references:
- Lapunzina P (2010). Sotos syndrome. Diagnostic and therapeutic protocols in pediatrics; 1:71-9.
(Updated at Apr 12 / 2024)